

Teamwork between cardiothoracic radiologists, interventional cardiologists and cardiothoracic surgeons.
Transcatheter Aortic Valve Replacement (TAVR) is percutaneous placement of prosthetic aortic valve under angiographic guidance. It is considered useful for patients with severe aortic valve stenosis, especially those at higher risk for open heart surgery. Recently, TAVR has also been offered to patients at intermediate or low risk for conventional surgery.
ECG-gated multislice CT plays an essential role in TAVR planning. It evaluates the aortic valve, aorta and iliofemoral arteries to ensure the selection of appropriate candidates, prosthesis types and treatment approach. A remarkable advantage of using ECG-gated CT for measurements of the aortic valve complex is its high reproducibility with excellent inter- and intrareader correlations.
The UCI CT protocol for TAVR consists of a combination of ECG-gated cardiac CT scan and whole-body CT angiography which allows for evaluation of the aortic valve, aortic root and coronary arteries and the luminal size. It also assesses tortuosity of the aorta and iliac or subclavian arteries for the TAVR procedure access planning. High spatial and temporal resolution of state of the art multislice CT scanners at UCI with 256 detectors and 0.27 second gantry rotation, and ECG-gating enable state-of-the-art evaluation of the aortic annulus. This CT scanners’ highly reliable depiction of the aortic valve and root anatomy allow for the appropriate selection of the valve prosthesis size which is of fundamental importance to prevent potentially postprocedural complications such as prosthesis embolization or para-valvular regurgitation.
The acquired TAVR CT protocol images are then postprocessed and analyzed by our subspecialty fellowship trained cardiothoracic radiologists using FDA approved dedicated cardiovascular imaging software. CT data are reconstructed into high- resolution axial, coronal and sagittal images and postprocessed multiplanar and 3D images with a structured report containing crucial measurements to aid the interventional cardiologist and surgeons during patient selection and procedure planning.
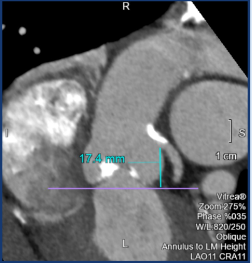

In the TAVR cardiac CT protocol, UCI cardiothoracic radiologists identify the reconstructed cardiac phase with the largest annular dimensions without motion artifacts from the multiphasic datasets to ensure precise measurements and appropriate device sizing. To accomplish this, they use retrospective ECG- gating scan with radiation dose modulation during systolic phase of the cardiac cycle, allowing for lower total radiation exposure. The imaging plane for the measurements is carefully selected because of the changes in the orientation of the annular plane throughout the cardiac cycle. Radiologists measure the aortic annulus luminal contour within plane at the most basal attachment points of the cusps of the three aortic valve leaflets. Important measurements include the annular area, diameters and perimeter which are larger in the systolic phase. The systolic assessment of the aortic annulus has been recommended in the recent guideline for avoiding unintended under sizing of the aortic valve prosthesis. Other important findings and measurements are the heights of the ostia of the coronary arteries, calcium score of the aortic valve and calcifications of the left ventricle outflow tract (LVOT).


In TAVR, CT is also the gold standard imaging modality for evaluation of the coronary arteries. Candidates of TAVR are usually older and have several risk factors of coronary artery disease. The ECG-gated CT scan allows for evaluation of coronary artery stenosis which is important in cases of severe aortic valve stenosis for the appropriate selection of treatments and precise risk assessment in TAVR candidates. Both, the cardiac ECG-gated CT and whole-body CT angiography components of the study are performed in seconds with a single intravenous administration of contrast media.
At UCI Medical Center, our mission for optimal care of TAVR patients goes even further, as we review every TAVR patient candidate clinical status and CT studies during a weekly multidisciplinary conference with our TAVR team of cardiologists, cardiovascular surgeons and cardiothoracic radiologists to ensure optimal patient selection and treatment planning. Teamwork between cardiothoracic radiologists, interventional cardiologists and cardiothoracic surgeons is essential for great outcomes in a TAVR program.
Pablo Abbona, MD